Female To Male (FTM) & Female To Nonbinary (FTN) Reconstruction Chest Surgery
Double Incision Top Surgery
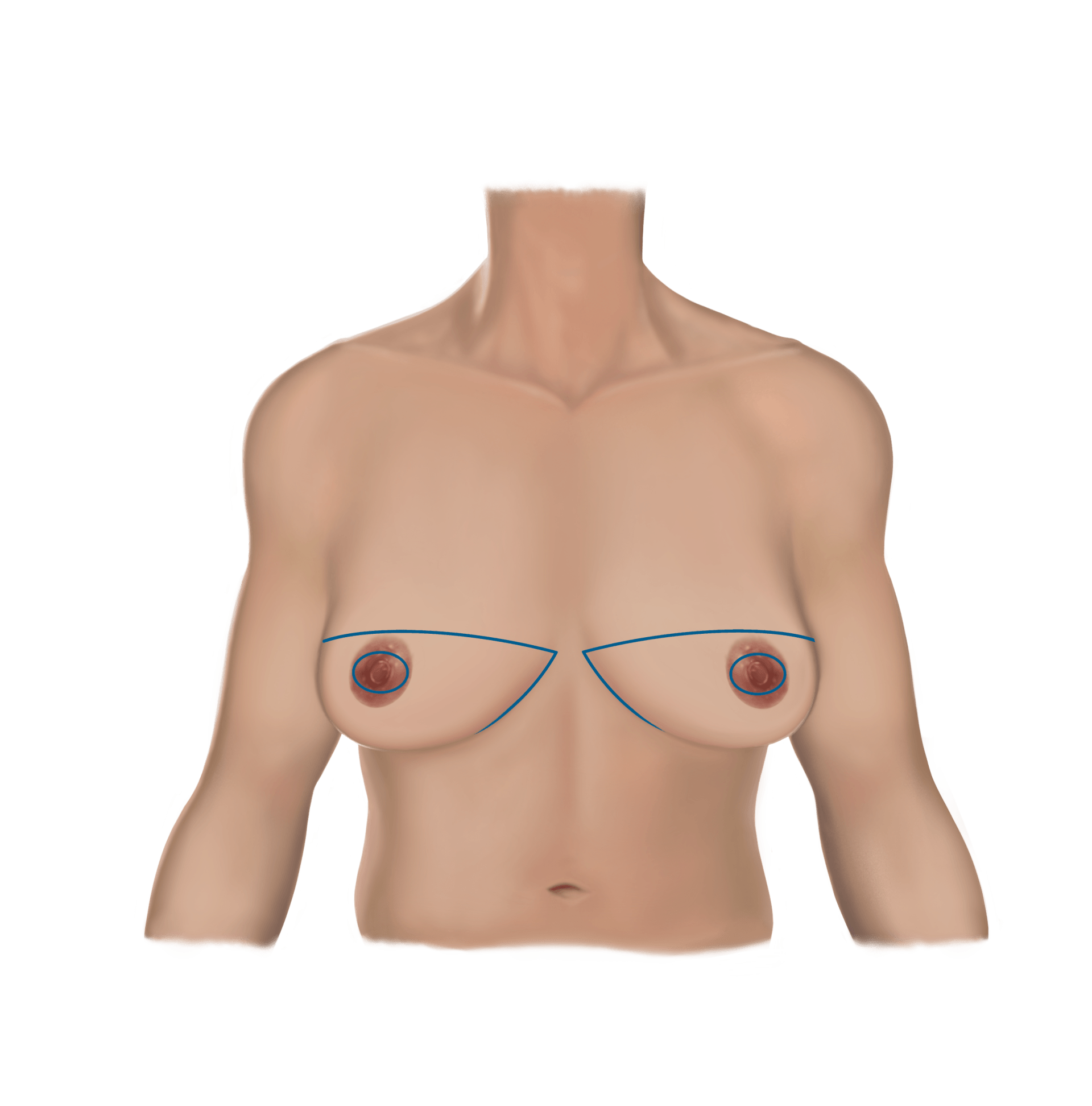
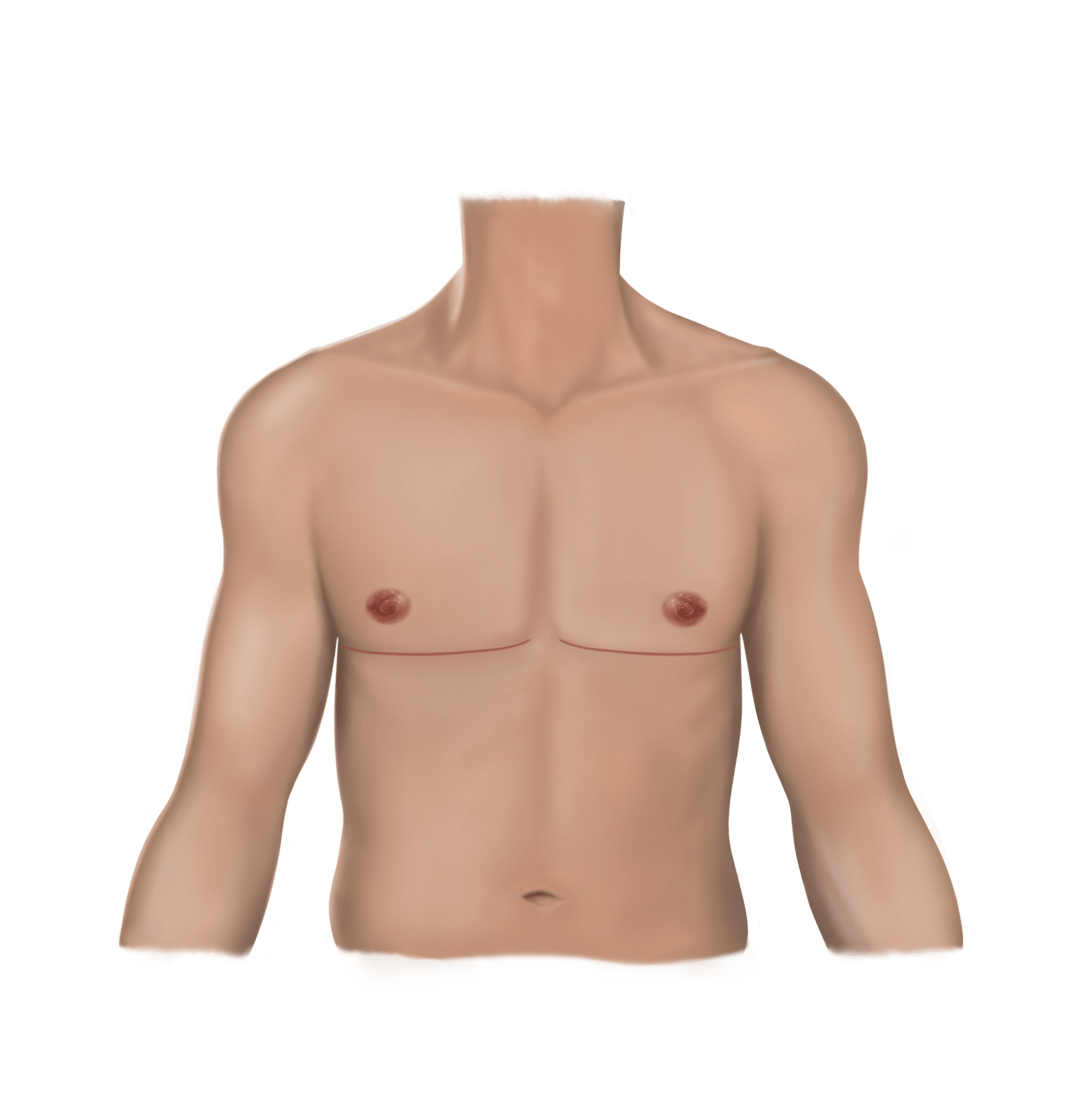
For patients with excess skin, a moderate to large volume of breast tissue or significant nipple ptosis, the Double Incision approach is most commonly selected. This approach is extremely effective at achieving the flattest possible chest wall, and it provides the most control over both chest wall contouring and nipple areola positioning. In some cases, liposuction is added to address fatty tissue that lies outside the borders of the previously existing breast tissue (the preaxilla, lateral chest wall or medial chest over the sternum).
This approach involves two incisions in an elliptical excision pattern, which results in a scar along the inferior chest border. There are various shapes to this scar which are discussed below. The nipples are removed and treated as “free nipple grafts”, which are resized, reshaped and replaced in a new location on the chest wall. This approach provides the most control over nipple areola positioning and allows for ideal chest wall contouring.
Free Nipple Grafts
“Free nipple grafts” means that the nipple areolas are removed, thinned out, reshaped and resized, and placed back on the chest wall. The areolas will become smaller and can be reshaped into an oval or a circle depending on your preference. This allows for maximal customizability in terms of size, shape, and location of the new nipple areolas. In addition, nipple projection is naturally reduced once the nipple grafts are created, which allows for natural deprojection of your nipple itself. If you have preferences regarding the size, shape, or location of your nipple areolas, you can communicate this to Dr. Chandler and these preferences can be incorporated into your surgical plan.
Scar Shapes–YOU HAVE OPTIONS!
The Double Incision approach is not performed with the same technique in every individual. There are different options regarding scar shape that can be customized depending on your preferences. While there are some restrictions based on anatomy, it is important to communicate your preferences to Dr. Chandler so your surgery can be tailored to your individual goals and needs as much as possible.
If you prefer a scar on the straighter side, Dr. Chandler may use an incision that is located 1-2cm higher than your inframammary fold, resulting in a very straight scar appearance. This is possible if your inframammary ligaments are not strongly inset along your inframammary fold. Another option is a scar that is gently curved and follows the natural anatomic chest wall boundary. This may be preferred by patients who do not desire such a straight line scar. A third option is a mix of the previous two, with a straighter scar across the middle of the chest that transitions to an outer upward curved scar. This results in a “contoured look” with the outer portion of the scar extending upward toward the armpit. This is an option for patients with out too much excess tissue in the lateral chest wall area (area under the armpit) because this technique does not allow for removing tissue in this area and may result in residual lateral fullness.
Nipple Characteristics
Similar to scar shape, you also have options when it comes to nipple areola size, shape and location on your chest wall. Many transmasculine patients opt for a nipple areola that is slightly off-center or laterally located and in the shape of a slight oval. Others opt for a circular nipple shape, and some have preferences regarding nipple areola diameter (on the smaller or larger side). The general range of nipple areola diameters generally ranges from 20-30 mm. There is some element of “vertical stretch” that occurs after surgery and is dependent on the amount of tension present on the inferior scar upon closing the incision, which Dr. Chandler may account for when determining your nipple areola measurements.
How the Procedure is Performed
The first step involved in this technique is removal of both nipple areola complexes as free nipple grafts followed by excision of an ellipse of skin and tissue at the lower chest border. This allows for removal of all the excess skin that is present, which does require a long incision that usually starts a few centimeters from the midline sternum and ends at the lateral chest wall, usually petering off where you see the breast tissue start to disappear laterally. In some patients, the central incisions are connected–this may be beneficial if your central skin folds are very close together, in order to avoid excess skin puckering or dimpling at the center of your chest. This incision allows the surgeon full visual access to the breast tissue and allows for excision of as much or as little tissue as desired. It also makes it easier for the surgeon to create an extremely uniform skin flap (the skin and tissue that will remain) which helps create a uniform appearance to the chest wall after surgery. After skin closure at the lower chest border is performed, the nipple grafts are placed back on the chest wall in the exact desired location, usually slightly lateral compared to that of a female nipple but can vary based on your preferences. The nipple areola grafts area also resized to the size of a masculine appearing nipple areola and reshaped into a slight oval or a circle (though theoretically another shape is possible such as a heart or a star).For an oval nipple areola, the dimensions of the new nipple areola are usually between 20-22mm in vertical height by 26-30mm in horizontal dimension.
Indications for the Double Incision Approach
- Large amount of breast tissue
- Significant skin excess
- Nipple ptosis (more than 1 cm)
- Desire for maximal chest wall flatness and maximal control over nipple areola complex positioning
The answer is not always straight forward. Patients with a moderate amount of breast tissue and some skin excess may find themselves falling within a borderline zone, where they could benefit from either a periareolar technique or a double incision or other skin excision technique. A full discussion during your consultation can provide some clarification.
Downsides to the Double Incision Approach
Nipple Numbness
Although this approach provides the most control over nipple areola positioning and chest wall contouring, the requirement for free nipple grafting carries inherent risks and unique benefits that are specific to this technique. The main risk involved in free nipple grafting is loss of nipple sensation. Because the nipple areolas are completely detached, they are freed of any nerve endings previously carrying sensation, and the nipple areolas will be 100% numb immediately after surgery. Peripheral nerves carry the intrinsic ability to repair and regenerate themselves, and so over a long period of time (months up to a year), nerve endings will very likely grow into the nipple grafts and will usually provide some return of skin sensation over time. It is important to note that this will not provide any hypersensitive or erotic nipple sensation, but will feel more like the surrounding normal skin. While the vast majority of patients do regain protective skin sensation to their nipple grafts, it is not a guarantee and there is still a small chance of permanent nipple numbness. If nipple hypersensitivity (erotic nipple sensation) is more important to you than chest wall flattness, you may want to consider an inverted T or buttonhole procedure as an alternative.
Nipple Hypopigmentation
Another inherent risk involved in free nipple grafting is hypopigmentation of the nipple areola. This is fairly common (about 25%) and usually results in mild discoloration (lighter pigmentation)in one area of the areola compared to another. However, this is easily correctable with a tattoo to correct and restore color to match the remaining areola pigment.
Nipple Graft Failure
A final risk involved in nipple grafts is theoretical graft failure, however this risk is extremely unlikely. With the correct technique involved in thinning the grafts prior to placement and creation of a well vascularized recipient site for the grafts on the chest wall, failure of the grafts could only feasibly result if the graft dressings were physically removed or significantly manipulated immediately after surgery, causing the underlying nipple grafts to shift from their original position. This is extremely unlikely to occur because the dressings that are placed over
the grafts are sutured in place, allowing the grafts to remain in place and heal underneath the dressings. It is important that the nipple grafts do not shift while they are healing because very tiny capillaries grow into the graft over the days following surgery, a step that is inherent to proper healing of the grafts. Bleeding underneath the graft is another possible reason for partial or total graft failure, which is prevented by a technique involving micropuncturing the graft to allow for fluid egress and controlling medications and external substances prior to
surgery which could negatively affect bleeding risk. Dr. Chandler has never lost an entire free nipple graft, however it is theoretically possible.
Length of the Scar
Some patients may be averse to the length of the scar that comes with the Double Incision approach. Avoiding the horizontal scar may be possible if you have a smaller volume of breast tissue and minimal skin excess. There is a small risk of poor scarring that comes with the longer horizontal scar, including hypertrophic, keloid or widened scarring. Hypertrophic and keloid scarring is very rare and more based on genetics, while widened scarring is possible depending on the amount of tension present on the skin closure. There is always some tension on the closure, and there are ways to prevent widened scarring by limiting the extent of arm raising after surgery as well as using scar therapy techniques to optimize your scar after surgery. See our
Postop Recovery Suggestions.
Summary
The Double Incision approach is a reliable, extremely effective way to achieve a flat chest wall, with multiple options regarding incision shape and nipple size, shape and position. The downsides are minimal and predictable and the satisfaction rates are high after surgery. It is important to carefully consider the downsides of this procedure and to consider your individual preferences and goals when deciding whether to have Double Incision top surgery.
Why Choose Us?

All Styles & Techniques
Double Incision, Keyhole, Peri, Buttonhole, Subglandular and Submuscular Breast Augmentation, Body Masculinization, Feminization and More

All Identities
Patients of all gender identities and all pronouns are welcome here

Individualized Care
We provide individualized care based on your specific surgical needs and goals and will inform you about your options

Book An Appointment With Us